First — why does the under-eye look that way?
A tired-looking under-eye is two things happening at once.
- A bulge — the fat that cushions the eye (orbital fat) pushes forward with age.
- A hollow — just below it, a dense, tough band called the tear trough ligament tethers the skin to the bone, creating a groove.
The step between bulge and hollow casts a shadow — and that shadow is what reads as dark circles and fatigue. In other words, the problem is not the amount of fat but its position, and the step it creates. If you remember one sentence from this article, make it that one.
Option ① Take it out — fat removal
For a long time, removing under-eye fat was treated as the standard. There's a bulge, so remove it — intuitive enough. But flattening the area by removal is far harder than it sounds.
- Even slightly too much leaves the area sunken — trading a tired look for a gaunt one.
- Reducing the bulge does nothing for the groove beneath it. Among patients who come to us for revision after removal elsewhere, we often find the bulge only somewhat reduced — and two steps remaining: the leftover bulge and the hollow groove.
- It may look fine when you're younger, but as facial volume declines with age, the removed area hollows out more visibly.
Option ② Fill it — filler
Then why not fill the hollow instead? The logic sounds right, but there's a structural problem.
That groove is not an empty space — it's a fold created by a ligament tethering the skin down. Filling "inside" the ligament is structurally difficult, and injected filler ends up spreading to either side of it. If the hollow is shallow, things may look better for a while; for a deep groove, it rarely solves the underlying problem.
One more thing — filler is said to fully dissolve with time, but what we see during surgery says otherwise. Operating on patients who had under-eye filler in the past, we frequently find it still present, or transformed into an altered, foreign-body-like material — even in patients injected ten years earlier. This residual filler blocks lymphatic flow, making post-surgical swelling last far longer.
Filler can buy a brief optical improvement. But the ending we see in clinic is usually the same — patients eventually come in for surgery anyway, and by then the residual foreign material has made that surgery considerably more demanding. This is also why we no longer offer filler at our clinic.
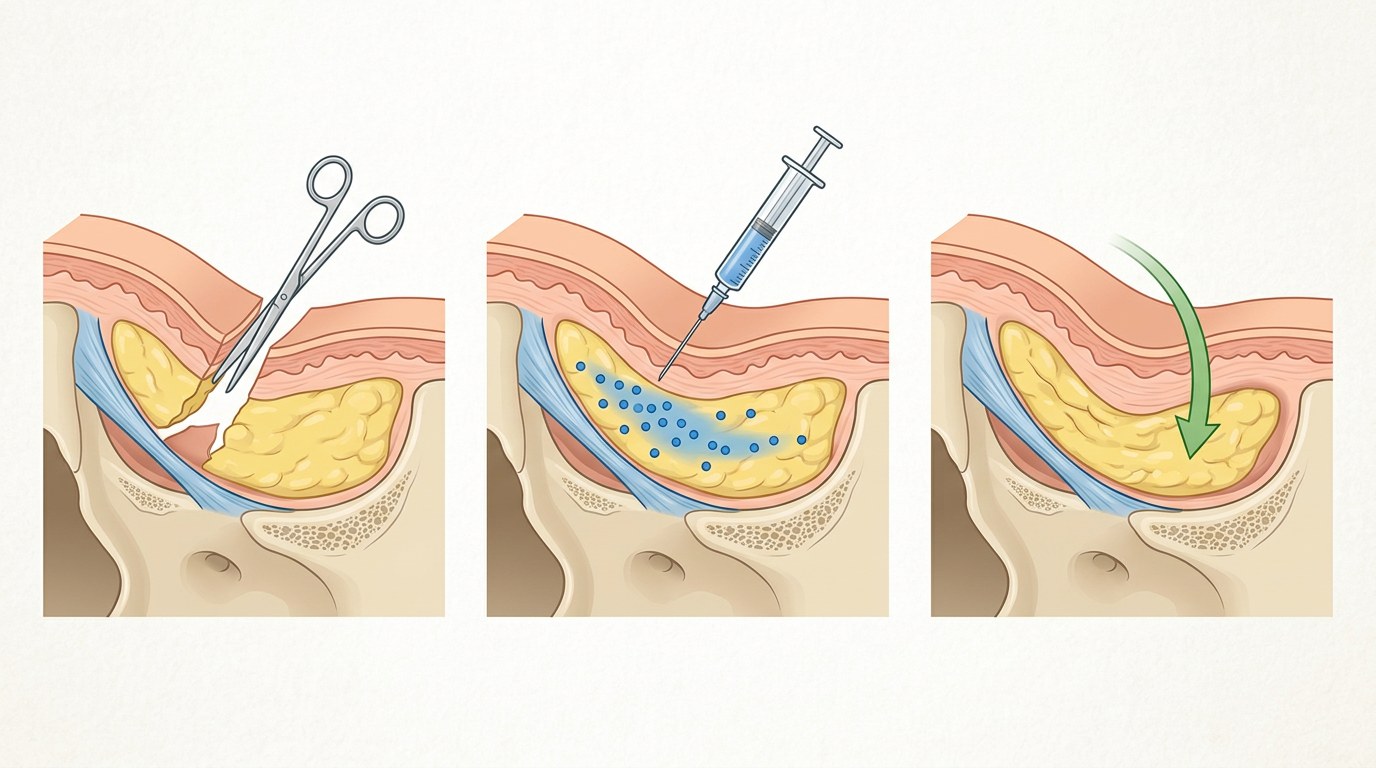
Option ③ Move it — fat repositioning
The logic of repositioning is simple: don't remove, don't add — relocate.
We release the tear trough ligament — the cause — and move your own displaced fat down into the groove to fill it. The bulge shrinks, the hollow fills, and the step between them smooths out. That is how the shadow disappears.
Rather than fighting an age-related change, repositioning uses it as material — which is why it's my default approach. And since it's your own fat rather than an implant or injectable, there's no foreign-substance issue.
The three options, one line each
| Principle | Limitation | |
|---|---|---|
| Removal | Take out the bulging fat | Groove remains · risk of hollowing |
| Filler | Fill the hollow with a foreign substance | Hard to fill inside the ligament · may persist/degrade |
| Repositioning | Release the ligament, relocate your own fat | It is surgery — recovery time needed |
Repositioning isn't a cure-all either — it is real surgery, with swelling and bruising to recover from, and results vary by individual. What sets it apart is that it's the only option that addresses the structure itself.
Diagnosis comes first
For some patients the cause is adhesion, which calls for a different approach again — see the real case of a patient told elsewhere that "it's muscle, it can't be operated on." And your history of filler and other procedures affects the surgical plan more than you'd expect, so please share it at consultation. Full procedure details are on our lower blepharoplasty page.
A few photos are enough for a remote assessment of which option fits you. Deciding among the three — that is where proper care begins.
※ Surgical methods and recovery vary by individual.
Need a consultation?
Reach us anytime via KakaoTalk, WhatsApp, or phone.